DIARRHEA AND MALNUTRITION
Prof. Ulysses Fagundes Neto
Esta
é a transcrição completa da palestra, por mim proferida a convite do professor
Fima Lifshitz, chefe do Serviço de Pediatric Research do North Shore University
Hospital afiliado da Cornell University Medical College, como saudação da minha
chegada para a realização do Pos-Doutorado em 1977.
It is well known that 2/3 of the children living in
the world are hungry and suffer some degree of malnutrition. Diarrhea is the
major cause of death in infancy in the underdeveloped countries and almost of
the children that died due to diarrheal disease had been malnourished.
Malnutrition and diarrhea are a binomial factor the
main component of a vicious cycle that is extremely hard to be broken, being by
this own reason the responsible cause of the high rates of mortality observed
in these children.
While for you (Americans) and for all the physicians
who work in the so-called developed countries malnutrition is almost always
secondary to diseases, such us malabsorption syndromes (Cystic fibrosis, Celiac
disease etc.), for me and for all the physicians who work in the underdeveloped
countries malnutrition is almost always a consequence of a socioeconomic
problem.
Overcrowding and wretched conditions where
promiscuity, contaminated environment, lack of water and sanitary supply,
associated to poor personal hygiene, with deficient formula intake, these are
the basic determinants of an unsteady state that can be tipped over, at any
moment, to a state of overt malnutrition.

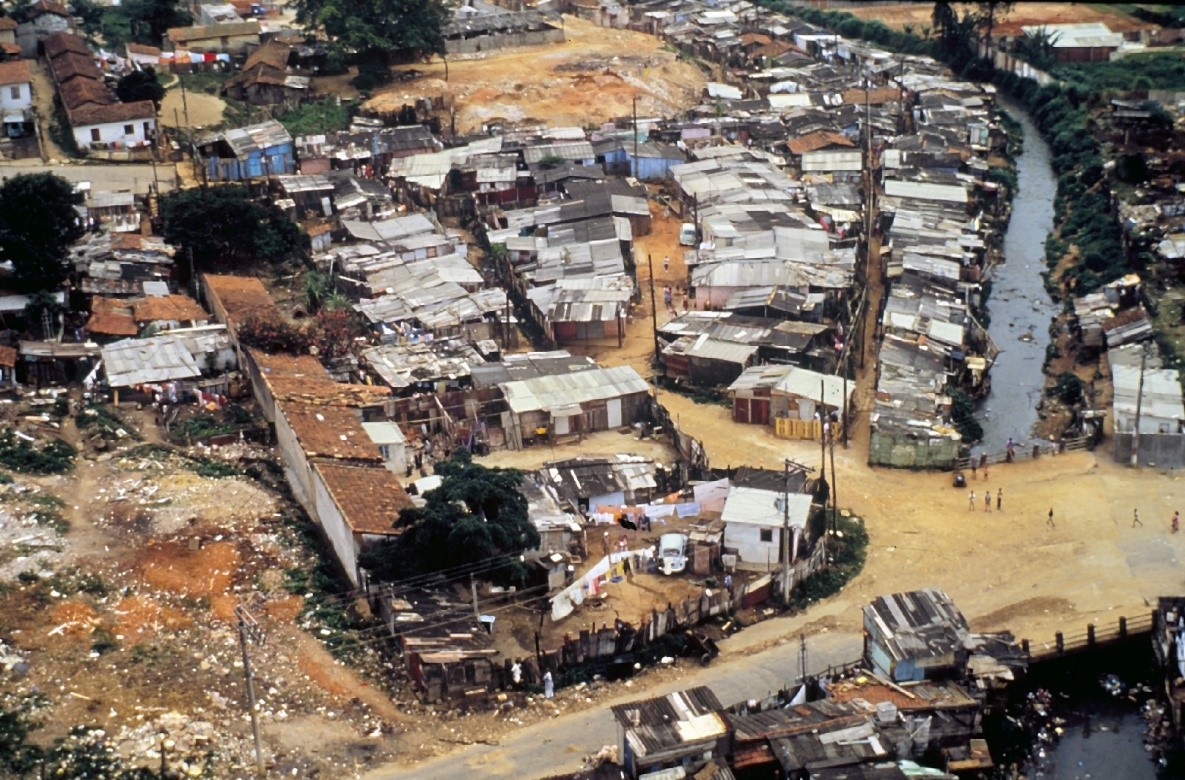
Vista aérea de uma fração da Favela Cidade Leonor.


However, at the time that we are involved with a
considerable number of malnourished children due to socioeconomic problems, we
must be alerted to correctly diagnose those children who are undernourished due
to secondary causes, like this seventeen-month-old child that came to us with a
history of diarrhea, weight loss and failure to grow for the last 5 months. A
daily fecal fat excretion of 12 grams and a D-xylose absorption with values of
12 mg% in the first hour and 9 mg% in the second hour, associated with total
villous atrophy in the small bowel biopsy practically made the diagnosis of
Celiac Disease. After receiving a gluten free diet for 6 months the clinical
appearance showed a complete nutritional recovery, with normal values of the
intestinal function tests, although there were still some mild alterations in
the intestinal morphology. This child, like several other children, could
easily been labeled as suffering from primary malnutrition in a more simplistic
approach and at this moment could be carrying all the undesirable stigmas of
malnutrition.
Este
foi o primeiro relato de caso publicado de Doença Celíaca (DC) com investigação
completa e recuperação clínica e nutricional em 1974 (Disciplina de
Gastroenterologia Pediátrica da Escola Paulista de Medicina).






The reason for secondary causes of malnutrition
associated to diarrhea within this large population of primary undernourished
children is one of the most important challenges in our daily medical practice.
Another striking difference between you and me, that
is, in the children that you must follow up and those that I must follow up is
related to the dietary scheme used in the first year of life. While for you it
may make no real difference at all whether the child is being breastfed or not,
to me this is a very important matter.
It has been well demonstrated that children while
exclusively breastfed, despite living in poor conditions, have a growth chart
very similar to those ones of the healthiest British children, but when human’s
milk is replaced by cow’s milk formula, or other new foods are incorporated to
the infant’s diet repeated infectious diarrheic episodes appear and
malnutrition supervenes. This is the classical picture known by the name of
“weanling diarrhea”.
To confirm this hypothesis which has been proven by
the classical studies in Punjab and in Guatemala, I invite you to follow me on
a long trip to a Brazilian Indian Reservation, called Xingu National Park. The
Reservation is in the heart of the country just on the beginning of the Amazon
region. The only means of transportation to reach this area is by plane.

Archeological studies indicate that the Indians
settled this area at least for the II century of our Era, and due to some
geographic peculiarities, the Indians remained in complete isolation until the
last years of the 19TH century. Nowadays these people are allowed to
live in their most natural way of living, and all their traditions, customs and
culture have been respected. They live in their little villages in houses built
by themselves.







Registro fotográfico da minha primeira viagem ao Parque Indígena do Xingu, em dezembro de 1970, semanas antes das solenidades da minha graduação em Medicina pela Escola Paulista de Medicina.
Their basic food supply are fish and starch obtained
from a special kind of root, called manioc, and wild fruits, mainly “piqui”, that
is rich in vitamin A.









Registro
das principais etapas do laborioso processo de elaboração do Biju
Breastfeeding is universal and the most important kind
of food during the first year of life, being practically the only nutritional
supply in this period of life, except for a special kind of juice made of
manioc and native fruits, that is offered near the end of the first year of
life. There is no other way to get animal milk since they have no pastoral
tradition, and so, human milk is the only option. Breastfeeding lasts
approximately until the third or fourth year of life and after weaning milk is
never again consumed by these population. In general, soon after the fifth year
of life the Indians become lactose intolerants due to a genetically lactase
deficiency acquisition.




To evaluate the nutritional status of the children
population below 5 years of age we have done a prospective study during 3
consecutive years. This study showed that the prevalence of malnutrition in
these children was 5.8% and despite malaria which is endemic in this region of
the country we did not find severe cases of malnutrition and the mortality rate
was very low. So, these people, some of the most primitive human beings still
alive, live in close relationship with nature showing a perfect state of adaptation
and integration. We can state by now that they do not demand any special medical
care, except of course for the routinary immunization schedule, to maintain
their nutritional status.







Este poster foi exposto, no mural do Carnegie Hall em Nova York, durante a temporada de concertos do cantor Sting em março de 1993, escrito em inglês e por mim vertido para o português. Vale ressaltar que Sting é um grande amigo do cacique Raoni desde longa data, e financiou parte da demarcação do Parque Indígena do Xingu.
On the other hand, when the descendants of these
people move up to our traditional western type of civilization, this happy and
healthy appearance gradually starts to disappear and becomes more difficult to
be seen in a considerable proportion of our general population. A clinical
picture of overt malnutrition can now be seen more frequently, and kwashiorkor
is one of the most common types of severe protein-energy malnutrition seen in
the rural zones of the country. However, when you reach the large cities, the
problems are multiplied, and the iceberg of malnutrition becomes more visible
in an earlier age.

These people original inhabitants of the rural zones
are attracted by the illusion of the great cities, and they constitute a
considerable migratory mass moving to the big urban centers. Most of these
families have numerous children and a very low income that compel them to live
in promiscuous environment with no potable water and lack of sewage system in
the periphery of the cities. Theses deleterious factors together with
precocious weaning predispose the children to suffer repeated episodes of
diarrheal diseases. Moreover, the high prices of formulas result on the
consumption of diluted preparation of the feeding bottles, thus contributing to
the aggravation of the nutritional status. Repeated infectious diseases,
frequent hospital admissions and deficient protein-energy intake are the main
factors of a vicious cycle that leads to severe protein-energy malnutrition in
the first five years of life and consequently to high rates of death. Marasmus
is the most common clinical picture of protein-energy malnutrition observed
among us.



Nutritional deficiencies of minerals, vitamins, protein,
and calories, associated to a contaminated environment, create a vicious cycle
that induce several alterations in the digestive system, mainly a malabsorption
syndrome. Currently, it is admitted that the alterations reported in the
digestive-absorptive function represent a summation of effects, among possible
others, between malnutrition itself and the changes observed in the intestinal
microbiota. Careful studies on pancreatic structure and function indicate that
the zymogen granules are decreased in the severe protein-energy malnutrition
and that after the stimulation with secretin and pancreozymin, pancreatic
output is also markedly reduced. The enzyme activity of the pancreatic output
is lower than normal, lipase, trypsin, chymotrypsin, and amylase being reduced
in that order.

In severe protein-energy malnutrition the intestinal
wall becomes thin and hypotonic, and the enteric mucosa can show histological
abnormalities in variable degrees of severity. In general, it can be said that
in kwashiorkor the villi aberrations although significant are non-specific.
However, some authors have shown severe alterations like those observed in
untreated celiac disease, in as many as 10-60% of the patients. The enterocyte
may show a cuboidal transformation and the mitotic index of the crypt cells
remains practically normal, while the crypt glands may be found to be
elongated.
In marasmus patients, on the other hand, the
morphological studies of the intestinal mucosa have shown controversial
results. Brunser et al. did not find significant changes in the small
intestinal morphology but have shown a low mitotic index in the crypt cells,
suggesting a low rate of cellular proliferation in the crypt glands. In our
experience, on the other hand, we have found alterations in varying degrees in
the intestinal morphology in 63% of the studied patients. In half of the
studied material the abnormalities were found to be non-specific, and we never
found total villous atrophy like that described in celiac disease. In 54% of
the patients, however, the small intestinal mucosa showed a very peculiar
morphological pattern of alteration that we called Diminished Villi Population.


Alterações
morfológicas da mucosa do intestino delgado com atrofia parcial das vilosidades
e aumento da distância entre elas, caracterizando população vilositária
diminuída (Tese de Mestrado por mim apresentada e aprovada com nota máxima ao
IBEPEGE em abril de 1977).



The digestive-absorptive function is impaired and
patients suffering from severe protein-energy malnutrition show steatorrhea and
a marked decrease in the D-xylose absorption test, the second hour being
significantly higher than the first hour. This observation may be due to a
delayed gastric emptying and/or intestinal hypomotility.
Dean et al, in 1952, were the first authors to
indicate the possibility of lactose or other carbohydrate intolerance in
malnourished patients. Disaccharidase deficiency, mainly lactase in up to 82%
of the patients and sucrase in up to 54% have been exhaustively reported in
malnourished children. The well-known deleterious effects of carbohydrate
malabsorption, therefore, can be seen not only to lactose intolerance, but also
with sucrose intolerance, and even in the more severe cases glucose
malabsorption have been described in the classical papers published by Lifshitz
et al. In our personal experience with marasmus patients 73% showed lactose,
23% sucrose and 5% glucose malabsorption.
A striking feature described in protein-energy
malnutrition is small intestine bacterial overgrowth. In normal condition the stomach,
duodenum and upper jejunum are practically sterile or have a sparce microflora
consisting predominantly of Gram+, facultative microorganisms, that are derived
from the oral cavity, colonizing the stomach and the upper bowel in a variable
wave like fashion following the meals. The distal portion of the ileum shows a
change of the flora composition with the appearance of Gam- microorganisms such
as coliforms and anaerobic Bacteroides. In the colon an evident change in the
number and types of microorganisms can be seen and of note is the increase in
the anaerobic population.
The acid gastric secretion, the secretory IgA
production, the bile salts, and the intestinal peristaltic movements are the
most important regulatory mechanisms that maintain the equilibrium of the
microflora, avoiding an abnormal bacterial overgrowth.
In protein-energy malnutrition most of these
regulatory mechanisms are deranged. Gastric achlorhydria, intestinal hypotonia
and hypomotility, and immunological deficiencies have been described in
malnourished children. These factors acting together with the lack of sanitary
environmental conditions will favor a chronic bacterial overgrowth in the small
intestine of these children. This bacterial overgrowth is considered one of the
most important causes of malabsorption reported in malnourished children.
The bacteria compete with the host for food and attack
proteins, folic acid, vitamin B12, nondigested carbohydrate, and for this
reason may provoke nutritional depletion in the host. Intestinal bacteria present in the upper
portions of the small intestine, especially the anaerobes, cause deconjugation
of the primary bile salts and 7 alpha dehydroxilation. The lowered
concentration of the conjugated bile salts together with the transformation in
secondary bile salts may result in fat malabsorption when they are reduced to a
concentration below the critical micellar level. The presence of deconjugated
and secondary bile salts in the jejunum otherwise defaulting fat absorption,
will damage the intestinal mucosa and impair glucose absorption by the
enterocytes. Bacterial proliferation into the jejunal lumen also competes with
the host in carbohydrate absorption causing fermentation with the production of
osmotically active particles increasing water loses leading to metabolic
acidosis.
In conclusion as you can see now it is easy to answer
why malnutrition and diarrhea constitute a binomial complex that come almost
always together and becomes easier to explain why the experimental conditions
not always reproduce the exact model observed in the clinical practice dealing
with malnourished children. The environment makes the whole difference due to
lack of sewage, no potable water supply, leading to contaminated foods, precocious
weaning, no hygienic education, numerous proles, low family income, all
together acting as the trigger factor of the vicious cycle
malnutrition-diarrhea. This binomial complex is one of the numerous challenges
that Health Care Professionals must face and try to solve in the underdeveloped
countries. Thank you.

Projeto
de implantação de promoção do aleitamento natural na comunidade da Favela
Cidade Leonor: uma profilaxia temporária retardando a ocorrência da Enteropatia
Ambiental (Teses de Mestrado em 1988 e Doutorado em 1993, de Fatima Lindoso,
por mim orientada apresentada ao curso de Pós-Graduação da Escola Paulista de
Medicina).
Nota de Esclarecimento
1- As fotos registradas nesse trabalho não coincidem necessariamente com a cronologia da palestra proferida, posto que a maioria delas foi obtida após o meu retorno ao país.
2- Toda a documentação fotográfica exposta nesse documento foi por mim realizada, exceto naquelas fotos em que estou presente.
3- A documentação fotográfica realizada no Parque Indígena do Xingu (PIX), foi registrada entre 1970 e 2000, intervalo de tempo em que trabalhei na referida área por meio de visitas anuais.
4- O trabalho de campo realizado na Favela Cidade Leonor tratou-se de um projeto de assistência e pesquisa da Disciplina de Gastroenterologia Pediátrica da Escola Paulista de Medicina (EPM), por mim coordenado, como parte do Programa de Pós-Graduação da nossa instituição, a partir de 1981, envolvendo Mestrandos e Doutorandos, e que resultou na elaboração de inúmeras teses de Mestrado e Doutorado.
5- A Favela Cidade Leonor foi erguida a partir dos anos 1950, às margens do córrego da Água Espraiada, o qual nasce na região do ABC e desagua no rio Pinheiros. Informações mais detalhadas deste trabalho de campo, estão descritas no Livro “Enteropatia Ambiental. Uma consequência do fracasso das políticas sociais e de saúde pública”, por mim escrito e editado pelo Editora REVINTER em 1996.